Early onset scoliosis (EOS) is a term that is currently recognized by pediatric orthopaedic and spine surgeons for patients presenting with scoliosis prior to 10 years of age. This type of scoliosis is rare. Children diagnosed with scoliosis are typically categorized by age into the following groups:
- Early Onset Scoliosis: 0-9 years old
- Adolescent Idiopathic Scoliosis: 10 -18 years old
Historically we have described patients with idiopathic scoliosis as having infantile (0-3 years), juvenile (4-10 years), and adolescent or adult onset scoliosis. The most common age to be diagnosed with scoliosis is in the pre-teen and adolescent years, when most of the child's thoracic growth is complete. EOS, however, is diagnosed at a very young age, requiring a very different treatment plan in order to accommodate the potential growth of the child.
Essential Anatomy
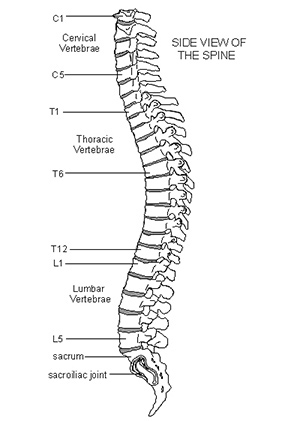 As with adolescent idiopathic scoliosis, early onset scoliosis can affect any region within the spine. From an anatomic and descriptive standpoint, the spine is divided into 4 general regions including the cervical, thoracic, and lumbar spine. The fourth region includes the sacrum and coccyx, which are essentially immobile and functionally part of the pelvis. In patients with early onset scoliosis, abnormal curves in the spine can occur in the cervical, thoracic, or lumbar spine and can span multiple regions of the spine including the pelvis. It is important to realize that scoliosis is a multi-plane, three-dimensional deformity. The spine can be curved abnormally side-to-side (coronally), but also front to back (sagittally). There is often rotation of the spine which may present as a rib hump. From an anatomic standpoint, smaller curves do not generally cause problems, but large curves can result in decreased room in the chest for the lungs and heart, decreased room in the spinal canal for the spinal cord or exiting nerve roots, or decreased room in the abdomen for organs.
As with adolescent idiopathic scoliosis, early onset scoliosis can affect any region within the spine. From an anatomic and descriptive standpoint, the spine is divided into 4 general regions including the cervical, thoracic, and lumbar spine. The fourth region includes the sacrum and coccyx, which are essentially immobile and functionally part of the pelvis. In patients with early onset scoliosis, abnormal curves in the spine can occur in the cervical, thoracic, or lumbar spine and can span multiple regions of the spine including the pelvis. It is important to realize that scoliosis is a multi-plane, three-dimensional deformity. The spine can be curved abnormally side-to-side (coronally), but also front to back (sagittally). There is often rotation of the spine which may present as a rib hump. From an anatomic standpoint, smaller curves do not generally cause problems, but large curves can result in decreased room in the chest for the lungs and heart, decreased room in the spinal canal for the spinal cord or exiting nerve roots, or decreased room in the abdomen for organs.
Causes
The underlying medical conditions of patients with early onset scoliosis help determine the prognosis and treatment. Some patients with neuromuscular conditions such as cerebral palsy or spina bifida have a very different treatment plan than patients without other medical problems. This is true even if the scoliosis appears similar in shape and size. In this section we will discuss a variety of conditions that are commonly associated with early onset scoliosis.
There are several sub-categories of early onset scoliosis that are commonly recognized. These include:
- Neuromuscular
- Syndromic
- Congenital
- Scoliosis associated with tumors, infection, and prior surgery or trauma
Neuromuscular Scoliosis
These are patients who develop scoliosis in association with conditions that affect their muscles or their nervous system. These might include the following:
- Muscular dystrophy
- Congenital myopathies
- Hypotonia
- Chiari malformation
- Cerebral Palsy
- Spina Bifida
- Charcot-Marie-Tooth disease
- Polio
Patients who are diagnosed with any of the conditions above may have higher rates of scoliosis, have an increased likelihood of a more progressive curve, and be less responsive to non-surgical treatments such as bracing or casting.
Syndromic Scoliosis
Syndromic scoliosis is associated with specific underlying syndromes and genetic conditions. Some of these conditions affect the bones, such as osteogenesis imperfecta (brittle bone disease). Other conditions affect connective tissues, such as arthrogryposis, Ehlers-Danlos syndrome, or Marfan syndrome. There is also a group of conditions associated with spinal deformities but it is not yet known how they affect the spine. These conditions include neurofibromatosis and a group of conditions called the mucopolysaccharidosis, which includes Hurler Syndrome.
Congenital Scoliosis
Congenital scoliosis is a deformity that is present before birth. In this condition, one or more bones in the spine are severely malformed or missing. This is not technically a subset of early onset scoliosis, but rather its own category. Spinal deformities in these patients have different treatments and prognoses based on the severity of deformation of the bone or bones, the pattern of deformity and whether the abnormal bones become more deformed as the child grows. Congenital scoliosis cannot be corrected with bracing or casting, however this type of treatment may be recommended for patients as a means to delay the curve progression and allow for growth and development prior to surgery. If the curve is large enough and/or worsening, there are very limited treatment options that don't involve surgery. Fortunately, many of these patients never get worse and therefore never need surgery. If your child is diagnosed with congenital scoliosis, it is also important that you request an evaluation of their kidneys and heart as these organs are formed at the same time as the spine and commonly present problems.
Idiopathic Scoliosis
Patients with idiopathic scoliosis have scoliosis without any of the other conditions discussed above or any other known reason. This is one of the most common forms of scoliosis in early onset scoliosis. Without treatment, the curve of the child's spine has a very high chance of progressing, causing many physical difficulties such as restricting lung development and function. Fortunately, idiopathic scoliosis seems to respond better to treatment than other forms of scoliosis and the chances of complications decrease with proper treatment.
Symptoms
Many children with early onset scoliosis look and function fairly normally. If the curves are mild, it can be very difficult to distinguish a child with EOS from children without a spinal deformity. The key to evaluating for a curve or curve progression is to pay close attention to symmetry:
- Shoulders should be level
- Shoulder blades should be the same height and shape
- Spine should run down the center of the back
- Head should be centered over the pelvis
- Head should be level
- Waist should appear symmetric
- Hips should appear level
- There should be no abnormal fullness in one side of the thoracic or lumbar spine on standing or when bent over at the waist
- They should not lean to one side
A thorough neurological exam is mandatory in the evaluation of any child with scoliosis, but this is especially true of children with EOS. When able, a complete sensory and motor examination should be performed with graded motor strength. Additionally, all major reflexes should be evaluated including abdominal reflexes. Back pain is generally not a significant complaint unless the curve is quite large. Likewise, numbness, weakness, or loss of bowel or bladder control would not normally be expected. If these symptoms do appear, emergent evaluation in the emergency department is essential.