Early onset scoliosis is important to treat for a number of reasons. The curves that these children have are often very aggressive and progress rapidly if they are not treated upon diagnosis. Aside from the obvious deformity and aesthetic issues, as the curves progress in magnitude they can deform the chest wall and can eventually cause problems with development of the lungs and other end organs. This can result in failure to gain height and weight, and in severe cases can result in decreased life expectancy. As a consequence, growth sparing treatments have been developed to try to control the progression of the deformity while allowing the spine to grow. Additionally, as these children reach skeletal maturity, many will need some type of definitive fusion of the spine to prevent progression into adulthood. Larger, stiffer curves that are not managed as children are very difficult to correct and are at a significantly higher risk of neurologic injury during these surgeries. By controlling the scoliosis earlier, the final curve correction is often better and almost certainly safer.
The evaluation and management of early onset scoliosis is a complex and evolving field. Caring for a child's growing spine with scoliosis is a dynamic and often unpredictable challenge. Significant advances have been made over the last decade and many more are on the horizon. As we better understand the nature of these curves, we hope to continue to make advances that will provide better outcomes for these children.
Non-Operative
Observation
In many cases, especially in infants, your child will initially be treated with observation. Your doctor will recommend follow-up appointments and x-rays to monitor your child. This is often done in order to determine whether the scoliosis will resolve on its own or if it will get worse over time. If it gets worse with observation, your doctor may recommend additional treatment.
Casting
 Casting is increasingly being utilized for the treatment of EOS. A cast is used to guide growth of the crooked spine into a straight spine, similar to how a crooked plant can be made to grow straight by tying it to a stake.
Casting is increasingly being utilized for the treatment of EOS. A cast is used to guide growth of the crooked spine into a straight spine, similar to how a crooked plant can be made to grow straight by tying it to a stake.
Application of a spine cast is done in a procedure center or operating room with your child under anesthesia. While under anesthesia the doctor is able to move their spine into better alignment before applying the cast. No incision is made during this process. This type of cast typically needs to be changed every 2-4 months. Some doctors place casts that go over the shoulder while others do not go over the shoulder. You can discuss these options with your doctor.
For some children casting is used as a means to prevent or delay progression of scoliosis. This may be recommended to allow children to grow as well as to increase lung development prior to surgery.
Bracing
Bracing is also used for management of early onset scoliosis. When compared with casting, there is less data on the effectiveness of bracing for EOS. Bracing is often used in conjunction with casting either during summer "breaks" or after your child's spine has successfully straightened with casting.
VEPTR & Growing Rods
VEPTR™
 VEPTR™ stands for vertical expandable prosthetic titanium rib. It is an FDA approved device that was developed to treat children with severe malformations of their chest and spine.
VEPTR™ stands for vertical expandable prosthetic titanium rib. It is an FDA approved device that was developed to treat children with severe malformations of their chest and spine.
VEPTR™ attaches to your child's ribs and either the spine or hip bone. It helps correct spinal and chest deformities without fusing the spine. Your child will usually need to have their device lengthened every 6-12 months by your doctor in the operating room. VEPTR™ has demonstrated effectiveness in management of early onset scoliosis, however, there are complications that can occur. These include infection, broken ribs, movement of implants, nerve injury, and prominence of the device causing pain. Ask your doctor about the specific risks and benefits for your child.
Growing Rods
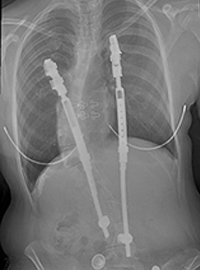
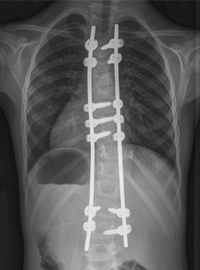
 Growing rods are surgical devices placed along your child's spine and attached to the spine with either hooks or screws above and below the curve. The area around the hooks and/or screws is fused to provide strong support. The curved part of the spine remains unfused. Similar to the VEPTR™, growing rods help correct spine and chest deformity and need to be lengthened every 6-12 months in the operating room.
Growing rods are surgical devices placed along your child's spine and attached to the spine with either hooks or screws above and below the curve. The area around the hooks and/or screws is fused to provide strong support. The curved part of the spine remains unfused. Similar to the VEPTR™, growing rods help correct spine and chest deformity and need to be lengthened every 6-12 months in the operating room.
They have similar risks to VEPTR™ including infection, movement of implants, nerve injury, inadvertent spinal fusion, and prominence of the device causing pain.
MAGEC™
 MAGEC™ rods are the newest type of growth-friendly device. They are implanted in the operating room in a similar manner to VEPTRs and growing rods. Surgeons can decide to pair this rod with other implant systems that attach to the spine including pedicle screws, hooks, wires, and anchors from the VEPTR™ system. An innovative and unique feature of MAGEC™ rods is that they may be lengthened with the use of an external magnetic controller allowing the patient to avoid an invasive procedure or even being placed under anesthesia. The surgeon and/or staff will perform the lengthening in the doctor's office. Due to the relative ease of the lengthening experience, many surgeons adopt a schedule of implant lengthening that is more frequent than the VEPTR and growing rods schedule of every 5-6 months. Risks of MAGEC™ rods include the risks associated with VEPTRs™ and growing rods in addition to failure of the mechanical aspects of the lengthening mechanism.
MAGEC™ rods are the newest type of growth-friendly device. They are implanted in the operating room in a similar manner to VEPTRs and growing rods. Surgeons can decide to pair this rod with other implant systems that attach to the spine including pedicle screws, hooks, wires, and anchors from the VEPTR™ system. An innovative and unique feature of MAGEC™ rods is that they may be lengthened with the use of an external magnetic controller allowing the patient to avoid an invasive procedure or even being placed under anesthesia. The surgeon and/or staff will perform the lengthening in the doctor's office. Due to the relative ease of the lengthening experience, many surgeons adopt a schedule of implant lengthening that is more frequent than the VEPTR and growing rods schedule of every 5-6 months. Risks of MAGEC™ rods include the risks associated with VEPTRs™ and growing rods in addition to failure of the mechanical aspects of the lengthening mechanism.
Vertebral Body Tethering
 Tethering attempts to straighten the spine by altering the growth of the spine without a definitive fusion. Screws are inserted on the outside of the vertebrae which connect a flexible cord along the spine. As the cord is tightened during surgery and as the child grows, the tether will help to adjust and straighten the curved spine. Tethering can often be done using small incisions in the chest utilizing a video camera. To learn more about this procedure, click here.
Tethering attempts to straighten the spine by altering the growth of the spine without a definitive fusion. Screws are inserted on the outside of the vertebrae which connect a flexible cord along the spine. As the cord is tightened during surgery and as the child grows, the tether will help to adjust and straighten the curved spine. Tethering can often be done using small incisions in the chest utilizing a video camera. To learn more about this procedure, click here.
Other Alternatives
Shilla™
 The Shilla technique involves doing a short spinal fusion at the most curved portion of the spine using screws and rods. The rods are then attached at the top and bottom of the spine to screws that allow for continued growth without manual lengthening. The Shilla technique remains experimental, with limited data about its effectiveness. The benefit of the Shilla technique is that if successful it does not require repeat trips to the operating room for expansion. Complications of the Shilla technique are similar to growing rods and VEPTR listed above. Availability of the special screws and rods needed for Shilla technique are limited in the United States. You can ask your doctor if they do the Shilla technique and if your child is an appropriate candidate for it
The Shilla technique involves doing a short spinal fusion at the most curved portion of the spine using screws and rods. The rods are then attached at the top and bottom of the spine to screws that allow for continued growth without manual lengthening. The Shilla technique remains experimental, with limited data about its effectiveness. The benefit of the Shilla technique is that if successful it does not require repeat trips to the operating room for expansion. Complications of the Shilla technique are similar to growing rods and VEPTR listed above. Availability of the special screws and rods needed for Shilla technique are limited in the United States. You can ask your doctor if they do the Shilla technique and if your child is an appropriate candidate for it
Stapling
 Stapling of the spine is a technique that acts like an "internal brace" for the spine and can help correct scoliosis through altering the growth pattern of the spine. A metal staple is inserted on one side of the curved spine to limit its growth. It can often be done through small incisions in the chest utilizing a video camera. The best patients for stapling are those with modest sized scoliosis who do not have rib and spine malformations. Stapling is not approved by the FDA and is only offered at a limited number of hospitals. Ask your doctor if they utilize this technique.
Stapling of the spine is a technique that acts like an "internal brace" for the spine and can help correct scoliosis through altering the growth pattern of the spine. A metal staple is inserted on one side of the curved spine to limit its growth. It can often be done through small incisions in the chest utilizing a video camera. The best patients for stapling are those with modest sized scoliosis who do not have rib and spine malformations. Stapling is not approved by the FDA and is only offered at a limited number of hospitals. Ask your doctor if they utilize this technique.
Alternative Techniques
There are many other proposed treatment methods for early onset scoliosis. These include chiropractic care, acupuncture, stretching, and massage. You may find various braces, medications, and exercise programs that propose to treat EOS. These various methods have not been scientifically studied and have not been demonstrated to show effectiveness in treating scoliosis. They often require significant out of pocket financial investments as well. Please ask your doctor about alternative techniques you are considering to help you make an informed decision about your child's care.
Definitive Fusion
In some cases, spinal fusion may be indicated for a child with early onset scoliosis. Most doctors have moved away from extensive spinal fusion for young children because it restricts chest and lung development.
There are certain cases, however, where a short fusion may be appropriate to try and prevent more serious progression of scoliosis. Short fusions are also done as part of the Shilla and growing rod technique.
A short fusion can also be done when a child has a hemivertebra, or malformed segment of the spine. This can be removed and replaced with a short fusion to help stabilize the spine. In many cases this can completely straighten the spine and prevent need for future surgeries. Your surgeon may do this all from one incision in the back, or may do an incision through the chest and the back. In most cases when a short fusion is done, your doctor will use screws, hooks, or wires to anchor to the spine. In some cases, however, they may choose to not use any anchors, often requiring your child to wear a cast after surgery for several months. This will help hold the spine in place while it fuses.
8.5.7